![]()
![]()
Aponeurotic variant of congenital ptosis: managed with levator re-insertion
Authors: Ankit Singh Tomar, Sameeksha Tadepalli, Sumeet Lahane, Raksha Rao, Santosh G Honavar
Abstract:
Purpose:
Description of congenital ptosis variant with aponeurosis disinsertion or dehiscence and their management with levator re-insertion.
Methods:
Retrospective review of patients with congenital ptosis with clinical features of aponeurotic dehiscence or disinsertion. Intra-operatively, careful hemostasis was maintained to ensure visualisation and identification of all layers. The levator palpebrae superioris (LPS) aponeurosis was identified before the pre-tarsal dissection, and it occasionally had a rolled up margin at it’s distal end. Re-insertion or advancement of the LPS aponeurosis was guided by the LPS action and amount of ptosis.
Results:
26 patients (mean age 24.6 ± 7.2years) were included. Severity of ptosis ranged from mild (18, 69.2%) to moderate (8, 30.8%). Majority had LPS action > 8 mm (22, 84.6%), with superiorly displaced eyelid crease in 10 (38.5%) and frontalis overaction in 7 (26.9%). None of the patients had eyelid lag in downgaze. 25 (96.15%) patients had undergone reinsertion and 1 (3.8%) had plication. Postoperative suture adjustment was done in 7(26.9%) and all patients had good post-operative results (symmetry between MRD1 of both eyes was ≤1 mm) at the final follow-up (mean+SD: 5.04+6.53m).
Conclusion:
Congenital variant of aponeurotic ptosis is less known entity and it is essential to differentiate it from congenital ptosis with dysgeneticlevator. All congenital ptosis cases with clinical signs of levator disinsertion deserve surgical exploration of the levator aponeurosis and repair of the aponeurotic defect. Meticulous intra-operative identification of layers of eyelid is imperative.
Introduction
Blepharoptosis is defined as an abnormally low-lying upper eyelid margin on primary gaze. Upper eyelid ptosis can be broadly classified as congenital or acquired. Congenital ptosis is characterised by poor levator palpebrae superioris action (LPSA), faint or absent lid crease and lid lag in downgaze, and results from myogenic development abnormality[1][2]. Other etiologies include a defect in the LPS muscle with fibrosis and decreased skeletal muscle fibers[3] and levator disinsertion secondary to birth trauma[4]. The aponeurotic acquired ptosis, which can be involutional, post-traumatic or associated with blepharochalasis, has good LPSA, superiorly displaced lid crease and no lid lag in downgaze. These features are also shared by aponeurotic variant of congenital ptosis, which is a less known entity discussed infrequently in literature[5][6]. It represents a mechanical defect of LPS, instead a dystrophy or maldevelopment, and is attributable to perinatal events such as trauma by forceps delivery, vacuum extraction and fetal rotation.We describe a series of 26 cases with congenital ptosis with aponeurosis disinsertion or dehiscence and their management with levator re-insertion.
Material and methods:
This retrospective review included allpatients withptosis of congenital onset, who had features of aponeurotic dehiscence or disinsertion. Preoperative evaluation included measurements of vertical palpebral fissure height, upper eyelid margin reflex distance (MRD1), levator palpebrae superioris muscle action (LPSA), severity of ptosis (mild: </= 2 mm, moderate: >2 and < 4 mm, severe: >/=4 mm), presence of lateral droop, assessment of frontalis overaction, ocular motility examination, eyelid crease height and nature(including number or a high, eyelid crease), lash ptosis and lid lag in downgaze.All preoperative and postoperative measurements (in units of 0.5 mm) were performed using a millimetre ruler. Pre and post-operative photographic documentation was done to compare the lid position and contour. The post-operative results were considered as good if the symmetry between MRD1 of both eyes was ≤1 mm; fair if 1.5 to 2.0 mm; and poor >2.0 mm.
Surgical technique
The anesthesia of choice for children was general anesthesia and frontal block (using 2% lidocaine and epinephrine) for adults. All patients were counselled for possible need for suture re-adjustment in case of under or over correction, within a week of surgery, on resolution of post-operative edema. The skin incision marked at 6-7 mm above the eyelid margin (based on the other eyelid margin crease distance to produce symmtery) and it was made with Radiofrequency ablation cautery. The dissection was carried out in the sub-orbicularis plane to expose orbital septum. The most crucial step intraoperatively was identification of disinserted levator aponeurosis which often showed a rolled over configuration with attachment to the orbital septum. Dehiscence or disinsertion of the levator aponeurosis was noted when the Müller muscle and conjunctiva—a translucent, reddish layer of muscle fibres and vertical parallel blood vessels —was clearly observed between the attachment site of the orbital septum and the upper edge of the tarsal plate[7]. The rolled up edge of aponeurosis is identified a white lineand gentle unrolling was carried out. The orbital septum wascarefully recessed to completely expose levator.The medial horn of levator was often found to be laxer than the lateral horn. The levator re-insertion was guided by levator action and amount of ptosis. A double armed 6-0 prolene suture is used to take 3-4 mm wide central horizontal lamellar bite of tarsus at midtarsal level and passed through disinserted end with similar oblique sutures at medial and lateral end. The sutures are tied one by one, while noting eyelid height and contour and suture tightness was titrated until adequate eyelid height was obtained.The dynamic eyelid crease formation suture (6-0 vicryl) incorporatedlevator and orbicularis and finally the skin was closed with 6-0 prolene. Post-operative medicine consisted of oral Amoxicillin-Clavulanic acid for 7 days and Moxifloxacin eye ointment for 2 weeks. In case of significant post-operative edema, systemic steroids were administered with rapid taper to aid in early resolution and assessment was carried out for need of suture adjustment.
Results
Patients’ data is summarised in Tables 1. Twenty four patients had unilateral ptosis (92%) and 2 had asymmetrical bilateral ptosis. Birth history was significant in 2 patients (history of prolonged labor). A large majority of patients had Levator action > 8 mm (22, 84.6%). A superiorly displaced eyelid crease was seen in 10 patients (38.5%) and three patients had a prominent lateral droop (11.5%). Intra-operatively, Twenty-one patients were found to havelevator disinsertion, one had levator dehiscence, and 4 patients had levator disinsertion with secondary fatty changes. None of the patients had eyelid lag in downgaze. Twenty five (96.15%) patients underwent levator re-insertion and 1 (3.8%) underwent levator plication. Seven patients needed postoperative suture adjustment (26.9%).All patients had good post-operative results with acceptable symmetry and cosmesis, with mean improvement in MRD 1 of 2.67 +/- 0.69 mm (Range- 1- 4 mm), at the final follow-up (mean+SD, range 5.04+6.53, 1 – 24 months).
Discussion:
We have herein reported the a case series of 26 cases with congenital ptosis with aponeurosis disinsertion or dehiscence and their management with levator re-insertion. This entity was first described by Anderson et al [5] in 1979 and subsequently by Martin et al[6] . Table 2 summarises the salient features in these studies in comparison to our data.
Three distinct variants of congenital aponeurotic ptosis could be identified and their features are summarised in table 3. Careful pre-operative evaluation and anticipating the type of mechanical defect will aid in the planning of management. Levator function is one of the key factors for determining the severity of blepharoptosis and selecting appropriate management. It is possibly affected by the amount of fatty deposit in the levator aponeurosis/LPS muscle because this deposit reduces the tractional force to the upper eyelid.
Our study was limited by several factors. First, this study had a retrospective design. The second limitation was the small sample size. A larger sample size with a prospective evaluation would be better suited in assessing the exact prevalence of this entity.
To conclude, congenital variant of aponeurotic ptosis is a less known entity and it is essential to identify and differentiate it from dysgenetic ptosis clinically. Such cases deserve careful surgical exploration of the levator aponeurosis and repair of the aponeurotic defect.
Table 1: Summary of patient data and measurement results
| Patients (number) | 26 |
| Male/female (numbers) | 8/18 |
| Right/left (numbers) | 14/12 |
| Age (range), (years) | 24.6 + 7.2 (5-37) |
| Preoperative MRD-1 (range), (mm) | 0.88 ± 0.71 (−1 to 2.5) |
| Levator function (range), (mm) | 11.38 ± 2.89 (6 to 16) |
| Margin crease distance (range), (mm) | 7.62 ± 2.02 (4 to 11) |
Table 3: Salient features of different variants of aponeurotic congenital ptosis
| LevatorDisinsertion | LevatorDehiscence | LevatorDisinsertion with fatty degeneration |
| Complete detachment of aponeurosis | Partial weakening of aponeurosis | Fat infiltration in detached aponeurosis |
| Vertical palpebral fissure reduced in downgaze | Normal palpebral fissure height in downgaze | Lid lag maybe seen |
| Good LPS action | Excellent LPS action | Good LPS action |
| High Lid crease | Normal/ High lid crease | Normal/ High lid crease |
| LevatorRe-insertion/ Advancement | Levatorplication | LevatorRe-insertion/ Plication/ Frontalis Sling |
Table 2: Comparison between different studies and their outcome in cases of congenital aponeurotic ptosis
| Martin et al[6] | Anderson et al[5] | Our Study | |
| Patients | 3 unilateral | 12 with 2 bilateral | 26 with 2 bilateral |
| Levator function | Excellent | Good- excellent | Good- excellent |
| Lid crease | High | Normal to high | Normal to high |
| Lid lag | Absent | Absent | Absent |
| Surgery | Exploration and Re-insertion | Exploration and Re-insertion | Exploration and Re-insertion |
| Results | All- cosmetically acceptable | 10- good results
2- LPS resection |
26- good results with no patient needing re-surgery |
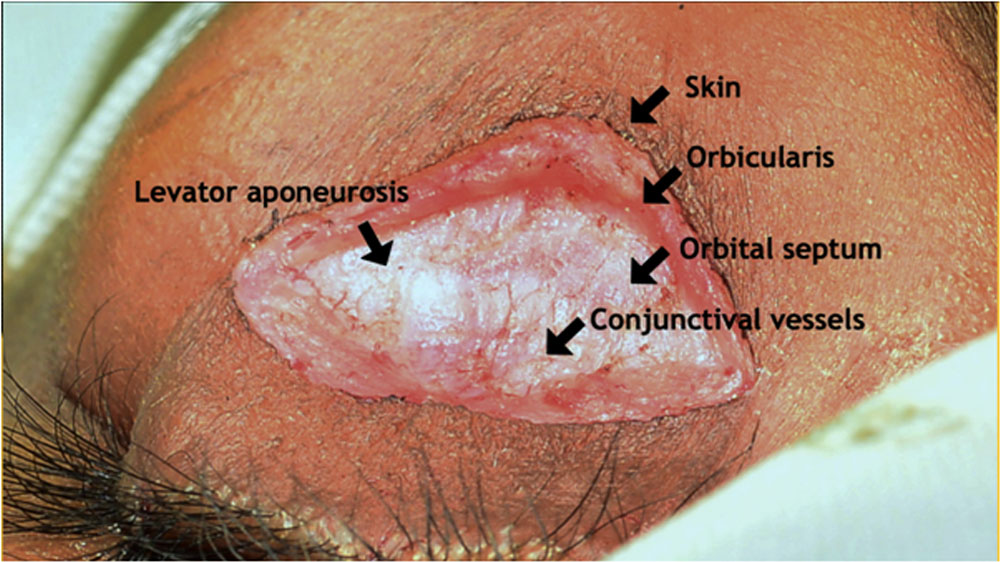 Figure 1 Intraoperative photograph showing detached levator aponeurosis appearing as a white band heralded by bare conjunctiva above tarsus
Figure 1 Intraoperative photograph showing detached levator aponeurosis appearing as a white band heralded by bare conjunctiva above tarsus
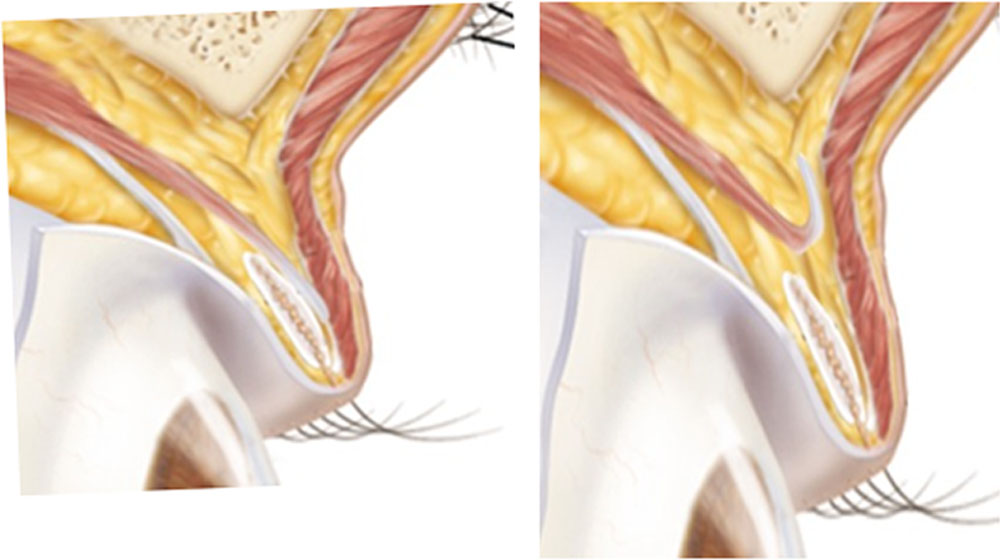 Figure 2 Schematic diagram showing detached levator aponeurosis and it’s rolled over edge
Figure 2 Schematic diagram showing detached levator aponeurosis and it’s rolled over edge
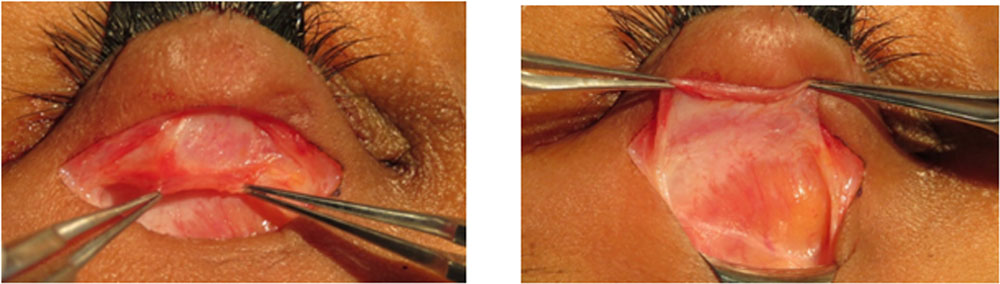 Figure 3 Intraoperative photograph showing unrolling of detached levator aponeurosis. Note the fatty infiltration of the levator muscle
Figure 3 Intraoperative photograph showing unrolling of detached levator aponeurosis. Note the fatty infiltration of the levator muscle
 Figure 4 Pre and Post operative pictures of a representative case of OS congenital aponeurotic ptosis. Note the improvement in high lid crease post-operatively.
Figure 4 Pre and Post operative pictures of a representative case of OS congenital aponeurotic ptosis. Note the improvement in high lid crease post-operatively.
Bibliography
- Griepentrog GJ, Diehl NN, Mohney BG. Incidence and demographics of childhood ptosis. Ophthalmology 2011;118(6):1180–3.
- Hashemi H, Khabazkhoob M, Emamian MH, Yekta A, Jafari A, Nabovati P, et al. The prevalence of ptosis in an Iranian adult population. J Curr Ophthalmol 2016;28(3):142–5.
- Lemagne JM, Colonval S, Moens B, Brucher JM. [Anatomical modification of the levator muscle of the eyelid in congenital ptosis]. Bull Soc Belge Ophtalmol 1992;243:23–7.
- Finsterer J. Ptosis: causes, presentation, and management. Aesthetic Plast Surg 2003;27(3):193–204.
- Anderson RL, Gordy DD. Aponeurotic defects in congenital ptosis. Ophthalmology 1979;86(8):1493–500.
- Martin PA, Rogers PA. Congenital aponeurotic ptosis. Aust N Z J Ophthalmol 1988;16(4):291–4.
- Cahill KV, Buerger GF, Johnson BL. Ptosis associated with fatty infiltration of Müller’s muscle and levator muscle. Ophthal Plast Reconstr Surg 1986;2(4):213–7.
Leave a Comment