Pediatric – I
Long term visual outcomes with Toric IOLs in pediatric eyes undergoing cataract surgery
The type of manuscript: Original Article
Title of the manuscript:Long term visual outcomes with Toric IOLs in pediatric eyes undergoing cataract surgery
Authors, in descending order, are as below:
Dr.Priyanka Patel, DNB, FREH
Dr.Vaishali Vasavada, MS
Dr.Lajja Shastri, MS
Dr.Shail Vasavada, DO, DNB
Dr. Deepa Agarwal, MS
Author Affiliations :
Raghudeep Eye Hospital, Ahmedabad, Índia
Total number of pages: 12
Total number of images: 2
Word count for the abstract: 123
Word count for the text: 2020
word counts for introduction + discussion: 222+765
correspondence address:
Raghudeep Eye Hospital
Gurukul Road, Memnagar,
Ahmedabad – 380052.
India.
Phone: 91-79-40400909
E-mail: info@raghudeepeyeclinic.com
Abstract:
Purpose:To evaluate long term visual outcomes following Toric IOL implantation in children with corneal astigmatism undergoing cataract surgery
Method:Prospective case series in 76 eyes of children with >1.5D of pre-existing corneal astigmatism undergoing cataract surgery and in the bag single-piece foldable Toric IOL implantation.Uncorrected and best corrected distance visual acuity(UDVA,BCVA) and residual refractive astigmatism measured at 12,24 and 36 months postoperatively.
Result:Mean age was 7.49(8-14) years.UDVA(LogMAR)improved from 0.54±0.15 preoperatively to 0.31±0.21,0.32±0.14 and 0.29± 0.20 at 12, 24 and 36 months respectively(p=0.0001).Meanastigmatism decreased from 1.49±2.08 D preoperatively to -0.04±0.65D,-0.17±0.65D and -0.25± 0.61D at 12,24 and 36 months postoperatively(P<0.001)
Conclusion:Toric IOL provides effective correction of astigmatism with excellent UCVA in paediatric cataract patients with pre-existing astigmatism which is sustained even at 36 months follow-up
Introduction:
Congenital cataract is a primary cause of childhood blindness which can be treated since many past years.1,2One of the factors affecting the outcomes of congenital cataract surgery is pre and postoperative astigmatism. Prevalence of pre-operative corneal astigmatism of >1.00 D in children with congenital cataract is approximately 79% (71.8% with the rule astigmatism).3This existing preoperative astigmatism influences postoperative refractive error after cataract surgery in children. Postoperative astigmatism has adverse effects on the vision development and can lead to amblyopia.4 One of the studies has reported mean astigmatism of around 5.8±3.6 D at 1 week after congenital cataract surgery.5 Type and location of incision and various suture characteristics like site, number, tightness etc are the various factors which can lead to postoperative corneal astigmatism.
In adults few months delay in the correction of postoperative refractive error will not affect the final visual outcome but in children precise refractive correction is needed immediately after cataract surgery. One of the ways to correct the preoperative corneal astigmatism is implantation of Toric IOL after congenital cataract surgery.
Outcomes of Toric IOLs have been extensively studied in adults. There are very few articles describing the results of Toric IOL in paediatric patients. In this study we are describing our longterm outcomes of Toric IOL implantation in paediatric patients with non-traumatic cataract and pre-existing corneal astigmatism.
PATIENTS AND METHODS
This prospective randomized study was carried out after approval by the Institutional Ethics Committee. The study followed the Tenets of the Declaration of Helsinki. Informed consent was obtained from the parents or guardian of the child after explaining all the alternatives regarding astigmatic correction techniques. Inclusion criteria were as follows:
(1) Children with visually significant developmental cataract associated with corneal astigmatism of more than 1.50D.
(2) Children in the age group of 8 years to 14 years who were cooperative for preoperative corneal marking.
Children with irregular astigmatism, traumatic or subluxated cataract, associated ocular abnormalities such as microcornea or buphthalmos and any macular pathology were excluded from the study. Each patient underwent a complete ophthalmologic examination including visual acuity (VA), slit-lamp examination, intraocular pressure (IOP) measurement by Goldmann’s applanation tonometer and dilated fundus examination by indirect ophthalmoscopy. Axial length was measured using partial coherence interferometry (IOL Master 500). Corneal astigmatism was determined using IOL master and manual keratometry. The spherical power of the IOL was then calculated using the SRK/T formula6, targeting emmetropia. Preoperative biometry, incision location and the surgeon’s estimated surgically induced astigmatism were used to determine the appropriate AcrySoftoric IOL model and axis of placement in the eye using an online calculator provided by the IOL manufacturer (Available from https://www.acrysoforiccalculator.com/; Figure 1). The corneal limbus was marked at the 0 degree and 180-degree positions after instilling topical proparacaine 0.5% in the conjunctival sac.
Surgical Technique
All surgeries were performed by the same surgeon (A.R.V.). A limbalparacentesis was created, and sodium hyaluronate 2.3% (Healon5) was injected in the anterior chamber. Two additional paracenteses were created at the 3 o’clock and 9 o’clock positions. A manual anterior CCC (ACCC) of approximately 4.5 to 5.0 mm was performed using a microincision capsulorhexis forceps under trypan blue staining in the absence of a red reflex. Bimanual irrigation/aspiration (I/A) was performed for lens removal, after which a 4 to 4.5 mm PCCC or pars plana anterior vitrectomy was performed. Thereafter, the temporal incision was enlarged and a single piece AcrySofToric IOL was implanted in the capsular bag.
All incisions were sutured with 10-0 nylon. After bimanual I/A for ophthalmic viscosurgical device (OVD) removal, Toric IOL is rotated to its desired axis of alignment and 0.1 mL of preservative-free triamcinolone acetonide (Aurocort) was injected intracamerally to detect vitreous strands and then washed out. An identical postoperative regimen consisting of topical antibiotic eyedrops (moxifloxacin 0.5%), prednisolone acetate (1.0%) eyedrops tapered over 3 months, and atropine sulfate 1.0% eyedrops for 2 weeks was followed in both groups.
Primary outcome measure was the difference in postoperative refractive cylinder at 1 year,2 years and 3 years. The secondary measures were comparison of pre- and postoperative visual outcome 1,2 and 3 years after the surgery.
Postoperative Examinations
All patients were examined postoperatively at 1 day and 1, 3, 6,12 months and then at 2and 3 years. Examinations included visual acuity, retinoscopy, keratometry (IOL master and Manual), applanation tonometry, detailed anterior and posterior segment assessment.
Statistical analysis:
Statistical analysis were performed using SPSS software (version 13, SPSS Inc.). The Student t-test was used to compare preoperative and postoperative refractive data. All statistical analyses were two-sided and P values less than 0.05 were considered statistically significant.
Results:
This study enrolled 76 eyes of 51 consecutive patients. Table 1 demonstrates the demographic profile of the patients. The mean age of the patients was 7.44±2.81 years (range 5–14 years). Mean corneal astigmatism was 1.46 ± 2.06 D (range 1.40–5.40 D). The mean spherical power of the toric IOLs was 21.54 ± 4.98 D (range 9.5-30.0 D) and the mean cylindrical power was 1.56± 2.76 D (range 1.50–6.00 D). Minimum follow-up period was 3 years.
Visual acuity:
Preoperatively, the uncorrected distance visual acuity (UDVA) was 0.54 log MAR ± 0.15 (range 0.20–0.80). The preoperative corrected distance visual acuity (CDVA) was 0.26 log MAR ± 0.25 (range 0–0.8). Postoperatively, at 6-month follow-up, mean UDVA and CDVA were 0.36 log MAR ± 0.18 (range 0.18–0.8) and 0.18 log MAR ± 0.19 (range 0.00– 0.48), respectively. At 1year follow-up,UDVA improved to 0.3 log MAR ± 0.21 (range 0.00–0.8) and CDVA improved to 0.13 log MAR ± 0.16 (range 0.00– 0.48). At 2 years follow-up, UDVA was 0.3 log MAR ± 0.14 (range 0.00–0.8) and CDVA was 0.28 log MAR ± 0.14 (range 0.00– 0.8) and at 3 years follow up UDVA was 0.29 log MAR ±0.2 (range 0.00–0.8) and CDVA was 0.25 log MAR ± 0.18 (range 0.00– 0.8). Therewas statistically significant difference between preoperative and postoperative UCVA and best corrected visual acuity (BCVA), respectively(p=0.0001 and p=0.03) at 3 years follow up (Table 2).
Refractive outcome:
Mean spherical equivalent (SE) was 0.8±1.05 D (range -2.25 to 3.75 D) at 6 months postoperatively. At 1 ,2 and 3 years the mean spherical equivalent was 0.86 ± 1.12 D (range -1.75 to 3.13 D), 0.63 ± 1.36 (range -1.75 to 3 D) and 0.64 ± 1.59 D (range -2.62 to 3 D) respectively.The mean refractive cylinder at 6 months, 1, 2 and 3 years postoperatively was -0.1± 0.66 D (range -1.5 to 1.25 D), -0.04± 0.65 D (range -1.0 to 1.50 D),-0.17 ± 0.65 D (range -2.0 to 1.0 D) and -0.25 ± 0.61 D (range -1.25 to 1.0 D) respectively.There was a statistically significant differenceinpre and postoperativeastigmatismat1 year follow up which was maintained till 3 years follow up (p<0.001).
Complications:
There were no intraoperative complications. We did not observe any significant rotation (>5°) in any case (Figure 2: showing Toric IOL with PCCC – 2 year follow up).Significant visual axis opacification was observed in 6 eyes at 2 and 3 years follow up visits for which yag laser capsulotomy was performed.
Discussion:
In this new era, it is possible to correct preoperative corneal astigmatism during the cataract surgery. Use of Toric IOL in adults having corneal astigmatism is a routine practice by all cataract surgeons. Now a days ToricIOLs are also being used in paediatric patients undergoing cataract surgery and having preoperative corneal astigmatism.
According to various data in literature regarding changes of astigmatism with increasing age, atypical child is born with against the rule astigmatism that decreases during the preschool years and results in with rule astigmatism during the school years. This astigmatism changes little during the early adult years, decreases gradually during the thirties and eventually becomes against the rule astigmatism.7,8
The corneal astigmatism changes the most from birth up to the age of 2 years and then decreases by 4-6 years of age and then stabilizes.9 Hence we have included patients between 8-14 years of age. Because of the unpredictability of corneal wound healing postoperatively corneal relaxing incisions are not a reliable option in paediatric patients.10,11Use of Toric IOL can play an important role in correction of corneal astigmatism in children undergoing cataract surgery.
Till now there is only one study published by Jagat ram et al12 comparing the use of ToricIOLs in children and there is one case report of use of bilateral Toric IOL implantation in a 16 years old child with Marfan’s syndrome.13
Many literatures have been published using Toric IOLs in the adults undergoing cataract surgery with pre-existing corneal astigmatism. Sheppard et al conducted a study in 67 eyes. In their study they could achieve UDVA of 20/40 or better in 88% of the eyes. The mean refractive cylinder also decreased significantly postoperatively from -1.91±1.07 D to -0.67± 0.54 D. They didn’t notice any significant change in keratometric cylinder.14 Ahmed et al15 performed a large prospective cohort study and the binocular UDVA was 20/40 or better in 99% of adult patients and 20/20 or better in 63% of patients, six months postoperatively. The mean residual refractive cylinder was 0.4±0.4 D, and 85% per cent of patients achieved a residual refractive cylinder of 1.00 D or less.
In our study, the mean preoperative UDVA (log MAR) was 0.54 log MAR ± 0.15(range 0.20–0.80) and CDVA was0.26 log MAR ± 0.25 (range 0–0.8), which was improved to UDVA of 0.29 log MAR ±0.2 (range 0.00–0.8) and CDVA of 0.25 log MAR ± 0.18 (range 0.00– 0.8) at 3 years follow up. Mean spherical equivalent (SE) was 0.64 ± 1.59 D (range -2.62 to 3 D) At 3 years postoperatively. The mean refractive cylinder was -0.25 ± 0.61 D (range -1.25 to 1.0 D) at 3 years postoperatively. In 96.05 % of the eyes had residual refractive cylinder of ≤1.00 D at 12 months postoperatively which was maintained even at 3 years follow up. Only 3 eyes had residual refractive cylinder of >1.00 D. The mean reduction in refractive cylinder is comparable to findings in previous studies in adults and indicates that the cylinder correction was effective.15 Results from recent studies have shown that the mean astigmatism of -1.92 ± 1.45 D preoperatively decreased to -0.67 ± 0.90 D at 2 years (73 eyes) postoperatively in adults.16
In our study, UDVA of 20/30 or better was achieved in 36.84% of patients andBCVA of 30/30 or better was achieved in 60.52% of the patients at 12 months postoperatively which was stable even at 3 years. These results are similar to the only study of Toric IOL in paediatric patients.12 Thus, patients with toric IOL implantation were comparatively less spectacle dependent. The major requirements for an optimal outcome of a Toric IOL are rotational stability and centration. Most IOL rotations occur in the early postoperative period that can be easily corrected with repositioning of the toric IOL in the desired axis. Once the anterior and posterior capsules fuse, rotation of the IOL is less frequent.17,18In our study refraction remained stable and showed stability of IOL without any significant rotation during the follow up period of 3 years.
Important limitation of our study was not taking into account the posterior corneal astigmatism which could have contributed to the residual astigmatism as we know automated keratometry method is biased towards overcorrection of with the rule astigmatism and under correction of against the rule astigmatism.19 The results of our study corroborate with previous studies carried out in adults who demonstrated that proper selection and preoperative examination of patients followed by uncomplicated IOL implantation of one-piece hydrophobic acrylic Toric IOLs resulted in acceptable stability and visual outcome.
Conclusion:
Toric IOLs provide effective correction of astigmatism with excellent UCVA in paediatric cataract patients with pre-existing astigmatism which is sustained even at 36 months follow-up. The Toric IOLs should be used in children of 8 years and above age group for better visual outcomes after cataract surgery and also to decrease the magnitude of amblyopia.
REFERENCES:
- Pi LH,Chen L, Liu Q, Ke N, Fang J, Zhang S et al . Prevalence of eye diseases and causes of visual impairment in school-aged children in Western China. J. Epidemiol. 2012. 22, 37–44
- Lim Z, Rubab S, Chan YH, Levin AV. Pediatric cataract: the Toronto experience-etiology. Am. J. Ophthalmol. 2010.149, 887–892
- Lin D, Chen J, Liu Z, Wu X, Long E, Luo Let al. Prevalenceof Corneal Astigmatism and Anterior Segmental Biometry Characteristics Before Surgery in Chinese Congenital Cataract Patients. Sci Rep. 2016 Feb 25; 6: 22092.
- Fulton AB, Dobson V, Salem D, Mar C, Petersen RA, Hansen RM. Cycloplegic refractions in infants and young children. Am J Ophthalmol 1980; 90: 239–247
- Spierer A, Nahum A. Changesin astigmatism after congenital cataract surgery and intraocular lens implantation using scleral tunnel incision. Eye (Lond). 2002 Jul;16(4):466-8
- Retzlaff JA, Sanders DR, Kraff MC. Development of the SRK/T intraocular lens implant power calculation formula. J Cataract Refract Surg 1990; 16:333–340; erratum,528
- Anstice J: Astigmatism–its components and their changes with age. Am J Optom Arch Am AcadOptom 1971; 48: 1001–1006
- Baldwin WR & Mills D: A longitudinal study of corneal astigmatism and total astigmatism. Am J OptomPhysiolOpt1981; 58: 206–211.
- Gwiazda J, Sheiman M, Mohindra I, Held R: Astigmatism in children: changes in axis and amount from birth to six years. Invest Ophthalmol Vis Sci 1984; 25: 88 –92.
- Troutman R, Swinger C: Relaxing incision for control of post operative astigmatism following keratoplasty. Ophthalmology 1980; 111: 117–120.
- Ben SG,Desatnik H: Correction of pre-existing astigmatism during cataract surgery: comparison between effects of opposite clear corneal incisions and single clear corneal incision. Greafes Arch Clin Exp Ophthalmol2005; 243: 321–326.
- Ram J, Singh R, Gupta R, Bhutani G, Gupta PC, Sukhija J. Toricintraocular lensimplantation in children with developmental cataract and pre existing corneal astigmatism.Acta Ophthalmol. 2017 Mar;95(2): e95-e100.
- Gimbel HV, Camoriano GD, Aman-Ullah M: Bilateral implantation of scleral fixated cionniendocapsular rings and toric intraocular lenses in a pediatric patient with marfan’s syndrome. Case Rep Ophthalmol2012; 3: 16 –23.
- Sheppard AL, Wolffsohn JS, Bhatt U, Hoffmann PC, Scheider A, Hütz WW et al.Clinical outcomesafter implantation of a new hydrophobic acrylic toric IOL during routine cataract surgery.J Cataract Refract Surg. 2013 Jan;39(1):41-7.
- Ahmed IIK, Rocha G, Slomovic AR, Climenhaga H, Gohill J, Gregoire A et al. Visual function and patient experience after bilateral implantation of toric intraocular lenses. J Cataract Refract Surg2010; 36: 609–616
- Miyake T, Kamiya K, Amano R, Iida Y, Tsunehiro S, Shimizu K. Long-term clinical outcomesof toric intraocular lens implantation in cataract cases with pre-existing astigmatism.J Cataract Refract Surg. 2014 Oct;40(10):1654-60.
- Linnola RJ, Sund M, Yl€onen R,Pihlajaniemi T: Adhesion of soluble fibronectin, vitronectin, and collagen type IV to intraocular lens materials. J Cataract Refract Surg2003; 29: 146–152.
- Lombardo M, Carbone G, Lombardo G, De Santo MP,Barberi R: Analysis of intraocular lens surface adhesiveness by atomic force microscopy. J Cataract Refract Surg2009 35: 1266–1272.
- Lijun Z, Mary ES, Harry M, Fei Y, Hamilton DR: Effect of posterior corneal astigmatism on refractive outcomes after toric intraocular lens implantation. J Cataract Refract Surg2015 41: 84 –89.
Table 1:
| Patients’ Demographic Data | ||
| Age (Mean±SD) (years) | 7.44±2.81 years (5–14 years) | |
| Gender | Male | 42.1 % |
| Female | 39.21 % | |
Table 2:
| Visual acuity preoperative and 6 months,1,2 and 3 years postoperative after AcrySoftoric intraocular lens implantation | |||||
| Preoperative | 6 months | 1 year | 2 years | 3 years | |
| UDVA
(LogMAR±SD) |
0.54 ± 0.15 | 0.36± 0.18 | 0.3 ± 0.21 | 0.3 ± 0.14 | 0.29±0.2(p=0.0001) |
| BCVA (LogMAR±SD) | 0.26 ± 0.25 | 0.18± 0.19 | 0.13±0.16 | 0.28±0.14 | 0.25±0.18(p=0.03) |
| CDVA, corrected distant visual acuity; log MAR, logarithm of minimum angle of resolution; SD, standard deviation; UDVA, uncorrected distant visual acuity | |||||
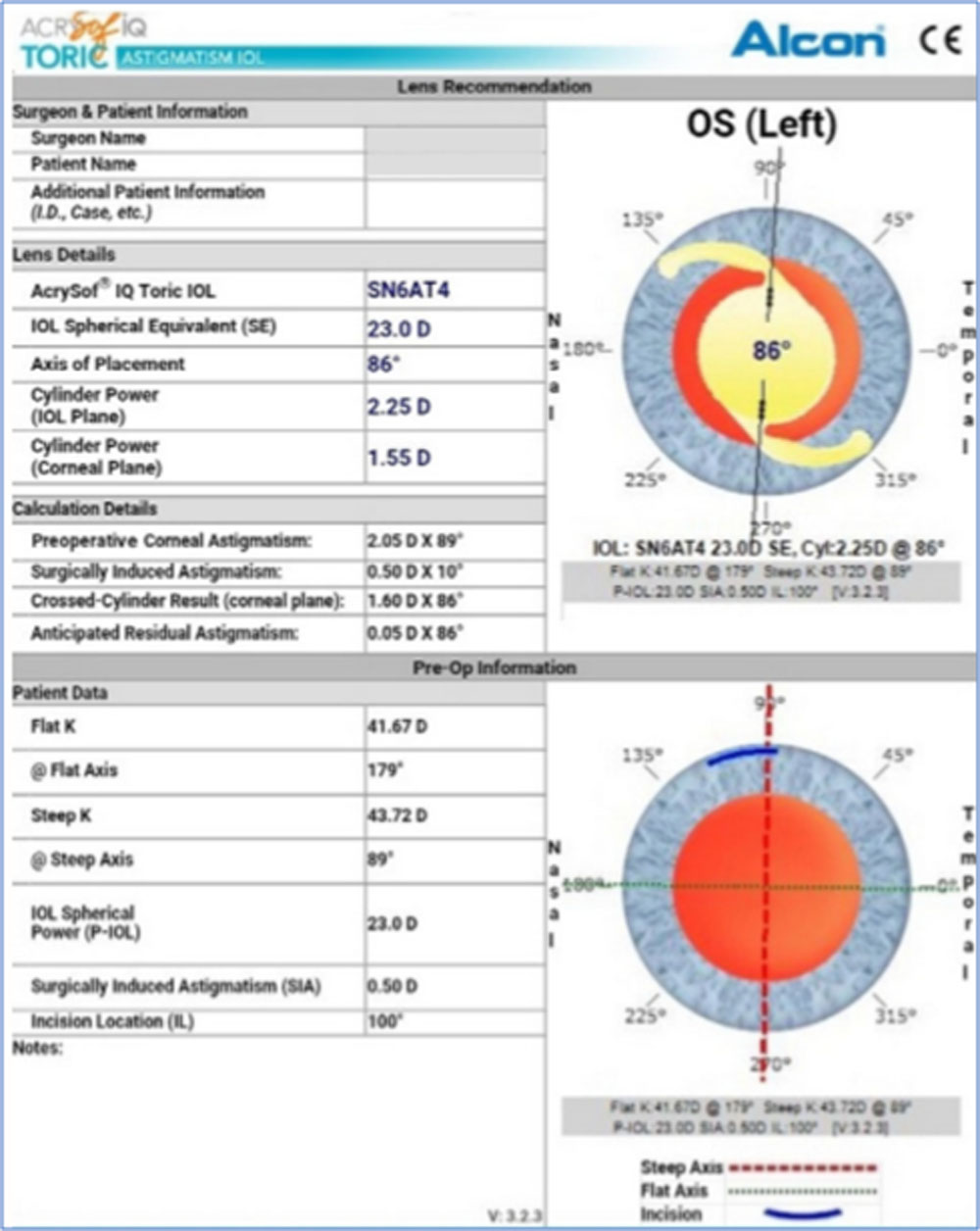
Figure 1: Preoperative toric intraocular lens (IOL) power calculation using an online calculator provided by the IOL manufacturer (Available from https://www.acrysoforiccalculator.com/).
 Figure 2: Toric IOL with PCCC – 2 year Follow up
Figure 2: Toric IOL with PCCC – 2 year Follow up
Leave a Comment